Shoulder Pain & Subacromial Impingement Syndrome
Suffer With Shoulder Pain?
How Common Is Subacromial Shoulder Impingement (SAIS)? How Common Is SAIS?
Do you struggle to lift your arm above your head or find yourself feeling a 'pinch' inside the shoulder joint during certain activities? If so, this post might prove useful. Shoulder complaints are the third common musculoskeletal presentation after back and neck disorders in primary care (8).
Shoulder impingement syndrome is a commonly diagnosed shoulder pathology and often presents in dominant than non dominant shoulders which tends to accumulate over a period of weeks to months (4, 5). The incidence of (SAIS) of all shoulder pain complaints account for approximately 44-65% and can cause a functional loss within the joint, making normal daily activities such as brushing hair or reaching up to objects or items painful (Michner et al., 2003) .
SAIS is Commonly found in people in individuals over the age of 40, their pain reports to be persistent and their cause can idiopathic without any known specific trauma.
The most common clinical diagnoses amongst shoulder complaints are rotator cuff muscle defects i.e. tears (85%) and/ or shoulder impingement syndrome (74%) (2). Changes in scapular kinematics (mechanics) that cause subjects to accumulate SAIS generally have decreased scapular posterior tilting, reduced upward rotation and increased internal rotation of the GHJ (5). Weak scapular musculature, fatigued infraspinatus and teres minor muscles are also associated along with changes of thoracic and cervical spine posture (8).
Rotator cuff muscle defects tend to increase with age as our joints reduce elasticity and flexibility and a considerable proportion
of individuals produce shoulder complaints over the age of sixty years old (3). Statistically, 30% of individuals over the age of 70 have a total defect within the joint but 75% of cases are asymptomatic (with reporting no symptoms) (3). People at this age group who do have subacromial impingement syndrome diagnosed tend to not receive international surgery.
Anatomy of the Subacromial Space
The subacromial space is defined by theHumeral head inferiorly, the under surface of the anterior third of the acromion, thecoracoacromial ligament and the acromioclavicular joint superiorly (figure 1).
The anatomical tissues within the subacromical space are the supraspinatus tendon, the subacromial bursa, the long head of biceps brachii tendon and the capsule of shoulder joint.Any one of the structures above can be affected and cause SAIS (4).
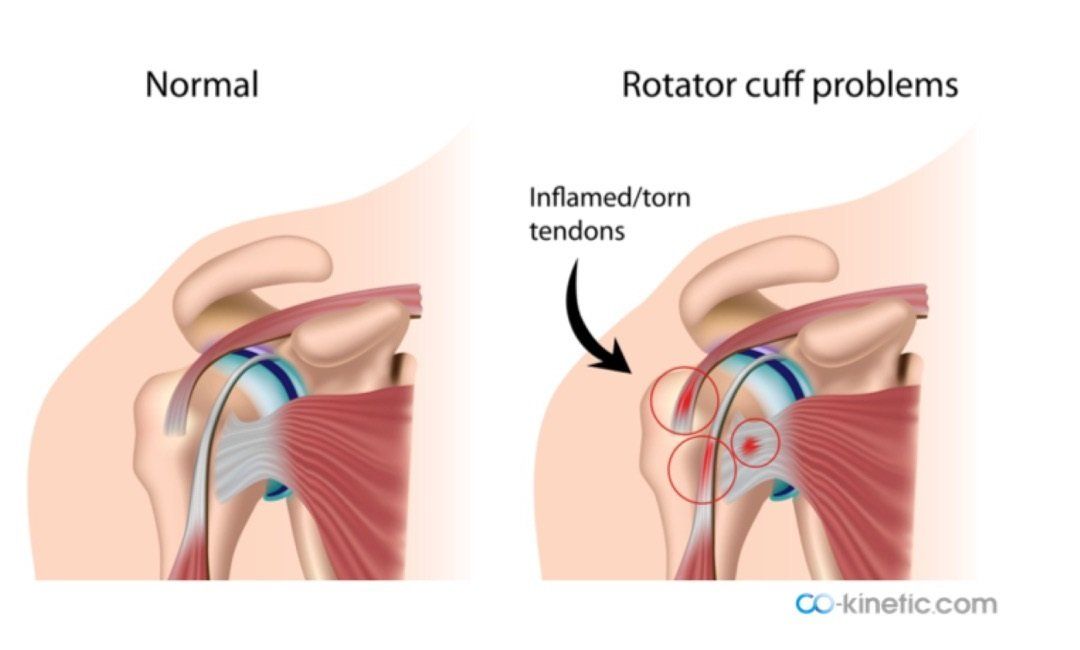
Figure 1
Primary and Secondary Impingement
Primary Impingement:
Primary impingement has been described by Neer as ‘impingement of the rotator cuff beneath the coracoacromial arch’ and is caused from structural changes within the joint which causes the subacromial space to narrow . This can be brought about from bony narrowing of the shoulder joint or increased volume (inflammation) of the subacromial soft tissues from e.g. subacromial bursitis or calcific tendonitis (3).
Primary impingement may result from subacromial crowding, posterior capsular tightness or excessive superior migration of the humeral head due to weakness of the humeral head muscle depressors.
Secondary Impingement:
Secondary impingement is a reduction of the subacromial space from scapulothoracic instability or a functional disturbance of the glenohumeral joint causing the centering of the humeral head with relation to the glenoid fossa to not be in the ideal position (3). It can be caused by a muscular imbalance leading to soft tissue entrapment or triggered by weakness of the rotator cuff muscle mechanism along with the biceps tendon (4). The end result of both syndromes is rotator cuff tendon inflammation and potential rupture if the same activities are performed repetitively.
Other Anatomical Factors
Anatomical factors that can narrow the subacromial space and cause 'pinching' of the rotator cuff (RC) tendons include:
1. Variations in shape of the acromion and its orientation of slope/ angulation which can be classified as flat (type I), curved (type II) or hooked (type III) (Figure 2) (8). There is uncertainty as to whether acromial shape is congenital or acquired with age (8).
2. Thickening of the coracoacromial ligament (figure 1) (8).
3. Reduced force output and muscle performance of the trapezius and serratus anterior muscles (8).
4. Weakness of rotator cuff musculature (8).
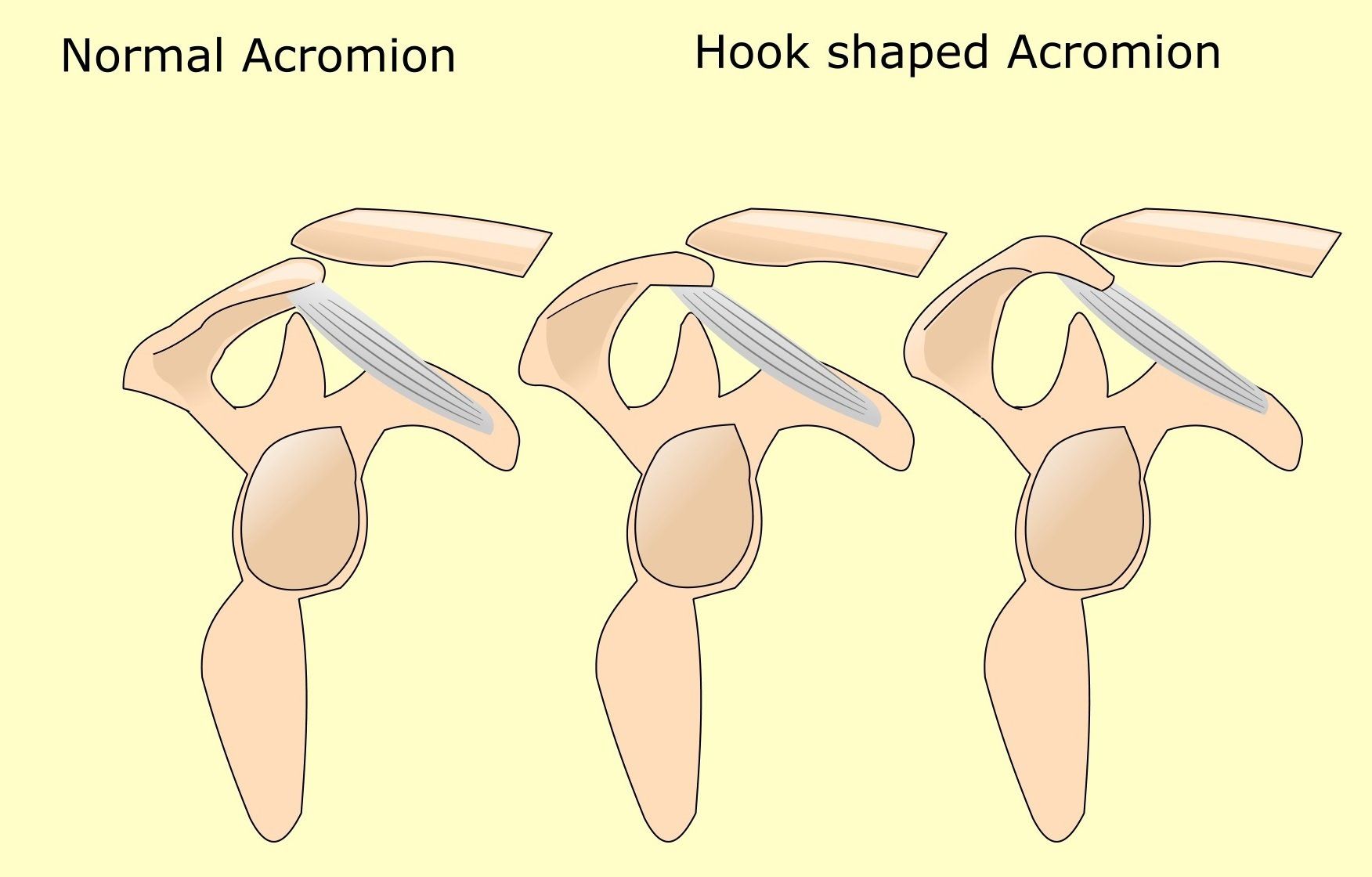
Figure 2
What Activities Commonly Make SAIS Worse?
SAIS is typically made worse by elevating the arm between 70 and 120 degrees, known as “painful arc” (Figure 3). Forced movement above the head and lying on the affected side.
What Can Be Done To Help?
Studies show that specifically designed exercise regimes prove to be the most successful method for helping patients with the condition (2, 7). BjornssonHallgren et al.,
(2017) discovered that specific exercises reduced the need for surgery in subacromial pain
patients after a 1 and 5-year follow-up.
Steuri et al.,
(2017) investigated the effectiveness of various different interventions including corticosteroids, nonsteroidal into anti-inflammatory drugs (NSAIDs), exercise manual therapy ultrasound laser shockwave therapy kinesiology tape myofacial trigger point therapy acupuncture and nerve block. They concluded that shoulder specific exercises proved to be most effective for patients with shoulder impingement. They also found that additional interventions such as manual therapy, tape, shockwave therapy and laser treatment might also benefit individuals rather than doing nothing to help improve symptoms (7).

2. Bjornsson Hallgren, H. C., Adolfsson, L. E., Johannon, K., Oberg, B. Peterson, A., Homgren, T. M. (2017) Specific Exercises for Subacromial Pain Good Results Maintained for 5 years,Acta Orthopaedica, 88 ;6: 600–605.
4. Kamkar, A., Irrgang, J. J., Whitney, S. L. (1993) Nonoperative Management of Secondary Shoulder Impingement Syndrome, Cinical Commentary, JOSPT,17; 5: 212-224.
5. McKenzie, T. A., Herrington, L., Horsley, I., Cools, A. (2015) An Evidence-Based Review of Current Perceptions with Regard to the Subacromial Space in Shoulder Impingement Syndromes: is it Important and What Influences it? Clin Biomech, 30; (7): 641-8.
6. Michener, L. A., McClure, P. W., Karduna, A. R. (2003) Anatomical and biomechanical mechanisms of subacromial impingement syndrome. Clinical Biomechanics; 18(5): 369–379.
7. Steuri, R., Sattelmayer, M, Elsig, S., Kolly, Tal, A., Taeymans, J., Hilfiker, R. (2017) Effectiveness of Conservative interventions including exercise, manual therapy and medical management in adults with shoulder impingement: a systematic review and meta-analysis of our RCTS, Br J Sports Med, 51: 1340-1347.